

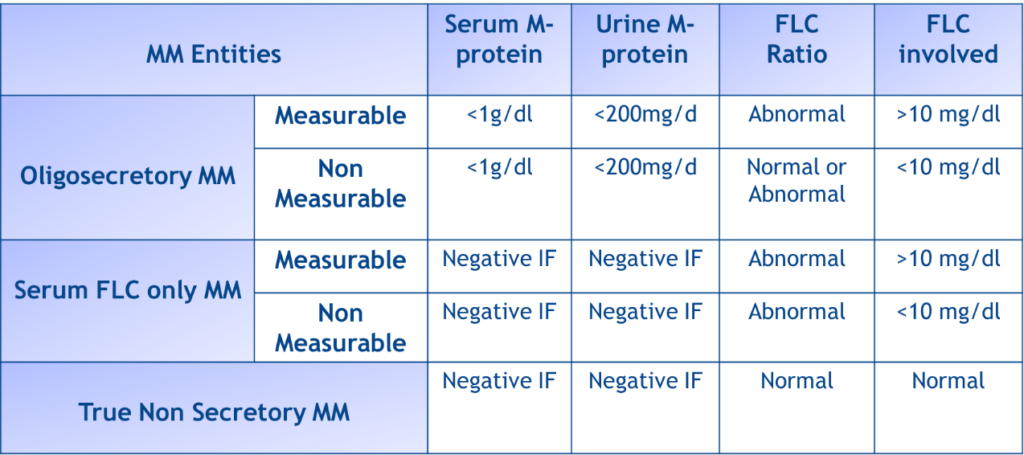
The first question is the nature of the second lesion. This is important for treatment decision. If it is plasmacytoma then the patient has true non-secretory myeloma (see the table below for the definitions of oligosecretory, light-chain only and non-secretory myeloma) and he needs anti-myeloma therapy. If the lesion is of another origin, then the patient needs treatment for the solitary plasmacytoma (radiotherapy only) plus therapy according to the nature of the second lesion. We biopsy the second lesion which was also plasmacytoma (add1q+ by FISH analysis of the plasma cells). Therefore, the patient has non-secretory multiple myeloma.
Another issue is the origin of the non-selective proteinuria and the cause of mild renal impairment. To exclude the presence of AL-amyloidosis we performed a fat biopsy which was negative for Congo red staining. Then we performed a kidney biopsy and the result was indicative of residual findings of previous acute post-infectious glomerulonephritis.
Based on the above, the correct answer is E: I am not sure; more tests are needed. The biopsy of the second lesion was needed to confirm the final diagnosis of true non-secretory multiple myeloma, while the kidney biopsy was needed to exclude AL-amyloidosis and to confirm the etiology of proteinuria and mild renal impairment (2% of AL-amyloidosis patients have no detectable free light chain with conventional methods).
Adapted by Dimopoulos MA et al. Oncology (Williston Park) 2013;27(9):930-932.
